Context: This editorial emphasize on ‘Ayushman Bharat Scheme’. The launch of this flagship health program i.e. Ayushman Bharat, in 2018, the Indian government has consistently emphasized the importance of enhancing medical accessibility, particularly in rural areas. This initiative aims to transform 150,000 public health centers (PHCs) into health and wellness centers (HWCs) to "bring healthcare closer to people's homes." It was evident from the beginning that achieving this goal would necessitate addressing the chronic shortages of doctors, frontline medical professionals, and healthcare infrastructure.
Given that healthcare falls under the purview of individual states in India, the central government's commitment to this endeavour necessitates a corresponding commitment from state governments. Unfortunately, most states that have traditionally lagged behind on welfare indicators have not adequately risen to this challenge.
The latest edition of the Centre’s Rural Health Statistics shows that the medical system outside urban areas continues to be plagued by a shortfall of doctors and infrastructure. Barely 45 per cent PHCs adhere to their mandate of functioning 24×7.A study published in The Lancet in February placed UP among the five states where district hospitals offer only 1 per cent of the basic services.
About Primary Health Centre (PHC)
- PHCs are the cornerstone of rural health services- a first port of call to a qualified doctor of the public sector in rural areas for the sick and those who directly report or are referred from Sub-Centres for curative, preventive and promotive health care
- The concept of Primary Health Centre (PHC) is not new to India. The Bhore Committee in 1946 gave the concept of PHC as a basic health unit to provide as close to the people as possible, an integrated curative and preventive health care to the rural population with emphasis on preventive and promotive aspects of health care.
- The Government of India's initiative to create and expand the presences of Primary Health Centres throughout the country is consistent with the eight elements of primary health care outlined in the Alma-Ata declaration.
Examples of primary health care services include routine check-ups, immunizations, screening tests, chronic disease management, and referrals to specialists when needed. Primary health care providers can include general practitioners, nurse practitioners, midwives, and community health workers.
Why primary health care is so important
- Promotes preventative care: Primary health care helps prevent illness and disease by promoting healthy living, encouraging vaccinations, and providing regular check-ups and screenings.
- Increases accessibility: Primary health care is often the most accessible form of healthcare, as it is typically delivered in local clinics or health centers that are close to where people live and work.
The share of primary healthcare in Current Government Health Expenditure (CGHE) has increased from 51.3% in 2014-15 to 55.9% in 2019-20. The increased focus on primary healthcare reinforces the government’s decisions to prioritize primary healthcare in the country.

- Reduces healthcare costs: Early detection and management of illnesses through primary health care can reduce the need for more expensive and specialized care, ultimately saving individuals and healthcare systems money.( It reduces the need for expensive secondary and tertiary healthcare.)
- Acc to National Health Accounts Estimates for India (2019-20)- Strengthening the PHC and focusing on preventive care will reduce the Out-of-Pocket Expenditure. The share of Out-of-Pocket Expenditure (OOPE) in total Health Expenditure (THE) declined from 62.6% to 47.1%. The continuous decline in the OOPE in the overall health spending show progress towards ensuring financial protection and Universal Health Coverage for citizens.
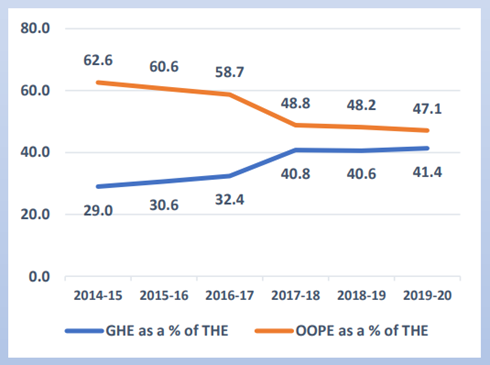
Figure 2: Government Health Expenditure and Out-of-pocket expenditure as % of Total Health Expenditure (%)
- Improves overall health outcomes: By providing comprehensive and continuous care, primary health care can help manage chronic conditions and improve overall health outcomes, including reducing mortality rates.
- Addresses health inequalities: Primary health care can help address health inequalities by providing equitable access to healthcare services regardless of income, race, gender, or location.
- Primary health related to Climate Change: Primary health care has an important role in responding to the climate change related threats to human health like injuries related to extreme weather events like storms, fires and floods; infectious disease outbreaks due to changing patterns of vector borne diseases; poor nutrition from reduced food availability because of drought; the psychological impact due to displacement of communities.
- Primary healthcare in developed nations: The majority of developed countries' federal healthcare budgets go towards primary care, including the UK, Australia, Canada, the Netherlands, and Sweden.
Problems of PHC in India
- Limited in scope- The existing primary healthcare model in the country covers only 15% of the health issues people seek care for, primarily related to pregnancy, limited childcare, and national health programs. Expanding its scope is essential for comprehensive healthcare coverage.
- Funding: The funding for general healthcare is quite low, leaving insufficient funds for primary healthcare.
| The central and state governments’ budgeted expenditure on healthcare touched 2.1 % of GDP in FY23 which was substantially lower that other BRICS countries (Brazil: 3.8%, China: 3.1%, Russia: 3.7%, South Africa: 4.2%) |
- Inadequate Infrastructure: According to the National Health Profile 2019 report, 22% of primary health centers do not have a separate room for immunization and family planning services.
| In Rajasthan, the population is often so dispersed (especially in hilly areas in the south and in the desert in the west) that a family may need to travel 10-20 km to reach the nearest PHC according to an analysis by the Centre for Economic and International. |
- Shortage of Healthcare Professionals: The delivery of quality health services is hampered by supply shortages, inadequate management, and the absence of proper training and supervision for healthcare workers. These issues can lead to interruptions in care, inefficiency, and outdated practices, all of which impact patient well-being.
| The rural healthcare infrastructure is three-tiered and includes a sub-center, primary health center (PHC) and CHC. Indian PHCs are short of more than 3,000 doctors, with the shortage up by 200% over the last 10 years to 27,421, as IndiaSpend reported in 2016. |
Lack of Access to Medicines:
The high cost of medicines is a significant barrier to healthcare access in India, with many people unable to afford even basic medications.
The government's free medicines program, which provides essential medicines to patients for free, has been plagued by shortages and supply chain issues.
The lack of access to medicines has led to many patients turning to unlicensed and unregulated pharmacies, which may sell substandard or counterfeit drugs.
Poor Quality of Care:
A study published in the Lancet found that around 50% of patients in India do not receive the appropriate care for their health conditions.
The lack of quality healthcare services is due to a range of factors, including a shortage of qualified healthcare professionals, inadequate infrastructure, and poor regulation of healthcare providers.
In addition, many patients in India lack awareness about their health conditions and may not seek timely medical treatment, leading to complications and poor health outcomes.
| An analysis by the Centre for Economic and International - India has a large network of primary health centres (PHCs), each supposed to serve a population of 25,000. In many poor states, such as Madhya Pradesh, Bihar and Jharkhand, however, a PHC covers as many as 45,000, 49,000 and 76,000 people. |
- Under-investment in primary healthcare : also means that PHCs continue to remain under-equipped and lacking supplies and drugs to provide comprehensive primary care.
| For example, of the 709 PHCs surveyed in 2009 by the International Institute for Population Sciences, Mumbai, about 24% did not have an electricity connection and 63% did not have piped water supply. |
At the same time, PHCs are expected to deliver centrally designed, targeted vertical programs, alienating them further from communities. As a result, even those families that can access PHCs continue to look elsewhere for their critical healthcare needs.
- Urban Neglect in Indian Healthcare System: The primary healthcare system in India has historically overlooked the growing urban population, as its focus has mainly been on rural areas. This neglect stems from historical policies and infrastructure designed for rural regions, despite the increasing urban population.
Way Forward
- Srinath Reddy committee recommendation: The High-Level Expert Group (HLEG) on Universal Health Coverage (UHC) headed by K. Srinath Reddy recommended that expenditures on primary health care, including general health information and promotion, curative services at the primary level, screening for risk factors at the population level, and cost-effective treatment, targeted toward specific risk factors, should account for at least 70% of all health care expenditures.
- Ayushman Bharat scheme seeks to upgrade more than 1.5 lakh health facilities like Sub Centres and Primary Health Centres to health and wellness Centres (HWC). These centres would deliver Comprehensive Primary Health Care (CPHC) bringing healthcare closer to the homes of people. This has to be implemented properly.
- Telemedicine: Telemedicine provides patients remote access to medical consultations and treatments via telecommunications technology. In turn, this contributes to closing the gaps in healthcare access, particularly in rural and remote areas. Telemedicine has proven to be a boon for Indians during the uncertain times of lockdowns, and it has the potential to make remote, optimized healthcare accessible to every corner of India in the future.
- Health Information Exchange (HIE): HIE systems enable the seamless sharing of patient health information between various healthcare providers, enhancing care coordination and substantially reducing medical errors.
- Mobile Health (mHealth): mHealth is an emerging concept involving the utilization of mobile devices and technology for health services, such as appointment scheduling, remote monitoring, and medication reminders. It can significantly improve patient access to care and treatment plan adherence.
- Government must increase budgetary allocations to healthcare to at least 3-4% of GDP so that public expenditure on healthcare is at least 70% of total health expenditure.


