Context: India's first patient diagnosed with Pompe disease, a rare genetic disorder, has passed away.
About Pompe disease:
It is a rare and progressive genetic disorder in which a complex sugar called glycogen builds up in the lysosomes (acellular structures that act as recycling center).
It is an autosomal recessive disorder, means when individuals with Pompe disease inherit two defective copies of the gene, one from each parent.
The disease occurs when individual, lack a specific digestive enzyme called acid alpha-glucosidase (GAA). The deficiency of GAA leads to the accumulation of glycogen in various tissues, particularly in muscles.
It is also known as glycogen storage disease type II (GSD II).
Symptoms of Pompe disease
Muscle weakness, difficulty breathing, respiratory insufficiency, enlarged heart (cardiomegaly), and problems with motor skills.
Diagnosis of Pompe disease
By genetic and enzyme test.
Cure of Pompe disease
There is no cure for the disease.
Treatment of Pompe disease
Involves enzyme replacement therapy (ERT), to replace the deficient GAA enzyme. The most commonly used enzyme in replacement therapy is alglucosidase alfa.
Cases in India:
Although no cumulative government data is available, there are about 50 individuals in India who currently suffer from Pompe disease.
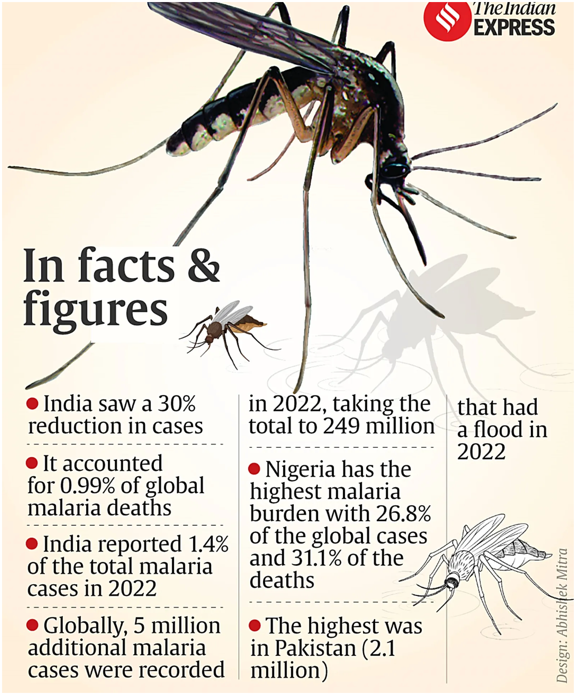
Context: In India there was an estimated 30 per cent decline in cases and 34 per cent decline in deaths compared to 2021 according to WHO’s World Malaria Report 2023.
Key findings of the report:
Globally around 5 million additional cases were recorded in 2022 compared to the 249 million cases in 2021.
The number of malaria deaths globally also remained higher than the pre-pandemic levels 608,000 deaths were reported in 2022 compared to 576,000 cases in 2019.
India accounted for 1.4 per cent of the global malaria cases and just 0.9 per cent of deaths.
Vivax malaria accounts for over 40 per cent of malaria cases in India.
Apart from India, Bangladesh, Bhutan, the Democratic People’s Republic of Korea, Nepal, Thailand and Timor-Leste also managed to reduce their malaria incidence by 55 per cent or more since 2015.
Africa was the worst-hit, with 94 per cent of all malaria cases and 95 per cent global malaria deaths in 2022.
Pakistan saw the largest increase, with about 2.6 million cases in 2022 compared to 500 000 in 2021. Significant increases were also observed in Ethiopia, Nigeria, Papua New Guinea and Uganda.
Climate change exaggerates the spread of malaria because the parasite is extremely sensitive to temperature, humidity, and rainfall.
About Malaria
About: It is a life-threatening disease caused by parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes. It is preventable and curable.
Transmission: Through blood transfusion, organ transplant, or the shared use of needles or syringes contaminated with blood because the malaria parasite is found in red blood cells of an infected person.
Types: There are 5 parasite species that cause malaria in humans, and 2 of these species: Plasmodium falciparum and Plasmodium vivax pose the greatest threat.
The vivax plasmodium is known to hide in the liver and cause recurrent infections.
Symptoms: Fever, chills, sweats, headaches, muscle aches, and fatigue. In severe cases, it can lead to complications such as organ failure and death.
Diagnosis: Through blood tests.
Antimalarial medications: Chloroquine, artemisinin-based combination therapies (ACTs), and others are commonly used, but drug resistance is a growing concern.
Prevention: To control the vector, insecticide-treated bed nets (ITNs) are used by endemic countries.
Vaccine: RTS,S/AS01 (brand name Mosquirix) and R21/Matrix M.
Path to malaria eradication: By WHO: Reducing case incidence and mortality rates by 75 per cent in 2025 and 90 per cent in 2030.
By India: Malaria-free by 2027 and to eliminate the disease by 2030.
Context: In the wake of the incident Silkyara Tunnel collapse , the Central Trade Unions have urged the Union government to ratify the labour conventions.
About Occupational Health & safety:
It is also known as workplace health and safety (WHS) or occupational safety and health (OSH), is a multidisciplinary field concerned with the well-being, health, and safety of people at work.
The primary goal of occupational health and safety is to create and maintain a safe and healthy work environment, preventing accidents, injuries, and illnesses related to work activities.
Key components of occupational health and safety:
Provisions for ensuring occupational safety in India:
Constitutional provision:
Article 39(e): The health of men, women and children should be protected, and children should be given opportunity and facility for healthy development.
Article 42: States that humane conditions at work and maternity relief should be provided.
International Labour Organization (ILO):
Labour Inspection Convention, 1947: To promote and improve labour inspection in various countries.
Labour Statistics Convention, 1985: On the standardization and improvement of labour statistics to facilitate international comparisons and promote informed decision-making in the field of labour.
World Day for Safety and Health at Work: It observed annually on April 28thfor promoting safe, healthy, and decent working environments and raising awareness.
Occupational Safety, Health and Working Conditions Code, 2020: To ensure that the workplace is free from hazards and provide free annual health examinations or tests, free of cost to certain classes of employees.
The Directorate General of Factory Advisory Services & Labour Institutes (DGFASLI): It serves as a technical arm of the ministry and assists in formulating national policies on occupational safety and health in factories and docks. It also advises factories on problems concerning safety, health, efficiency and well-being of every employee.
Challenges related to occupational health and safety:
Inadequate safety measures: Instances like Silkyara Tunnel collapse underscore the risks they face, including building collapses and industrial accidents due to inadequate safety measures.
Lack of doctors: On the various occupational diseases and workplace hazards and risks.
Data related to few sector: Labour Bureau compiles and publishes data on industrial injuries relating only to a few sectors, viz. factories, mines, railways, docks and ports.
Lack of regulatorycompliance : For registered factories nationwide decreased from 36.23% in the period of 2008-11 to 24.76% in the fiscal year 2019-20.
Inadequate human resource: For effective monitoring like in Major States such as Maharashtra (38.93%), Gujarat (57.52%), Tamil Nadu (58.33%), and Bihar (47.62%) had poor employment rates of inspectors.
Way forward to strengthen occupational health and safety:
India should ratified ILO Occupational Safety and Health Convention to promote and ensure the safety and health of workers in the workplace.
Setting up emergency standards for hazardous company in India under Occupational Safety, Health and Working Conditions Code.
Establishment of Occupational Safety, Health (OSH)committees and involve workers for identifying hazards and improving OSH.
The labour codes, especially the OSH Code, the inspection and the labour statistical systems need to be reviewed as the Government is in the process of framing theVision@2047 document for the Labour Ministry.
Key findings of ‘A Call for Safer and Healthier Working Environments’ report by the International Labour Organization (ILO):
Over 63% of fatalities occur in the Asia-Pacific region, primarily attributed to the absence of a robust safety net.
Threats to workers: Long working hours, exposure to particulate matter, gases, and fumes, and occupational injuries are major causes. Mining, construction, and utilities are the most hazardous sectors.
The health of the workers has several determinants, including risk factors at the workplace leading to cancers, accidents, musculoskeletal diseases, respiratory diseases, hearing loss, circulatory diseases, stress related disorders, communicable diseases and others.
Context: Health Ministry has made available generic drugs to support the care and treatment of four ailments: Tyrosinemia-Type 1, Gaucher’s Disease, Wilson’s Disease, and the Dravet-Lennox Gastaut Syndrome.
About Rare Diseases:
It is a debilitating lifelong disease or disorder that occurs infrequently in the human population.
WHO defines rare disease with a prevalence of 1 or less, per 1000 population.
There is no universally accepted definition of rare diseases India accept that a disease prevalence of less than 100 patients per 100,000 people is categorized as a rare disease.
A rare disease, also referred to as an orphan disease, is a health condition that affects a small number of people compared to the general population.
These diseases can be genetic or acquired.
Some examples of rare diseases include Huntington's disease, cystic fibrosis, amyotrophic lateral sclerosis (ALS), Haemophilia, Thalassemia, Sickle-cell Anaemia, Cystic Fibrosis, auto-immune diseases and others types of muscular dystrophy.
Due to the limited number of affected individuals, research and development for treatments may be insufficient, and patients may face difficulties in obtaining a timely and accurate diagnosis. The rarity of these diseases often makes it challenging to conduct clinical trials, gather data, and develop effective treatments.
Tyrosinemia-Type 1: It is a rare autosomal recessive genetic metabolic disorder characterized by lack of the enzyme fumarylacetoacetate hydrolase (FAH) which is needed for the final break down of the amino acid tyrosine.
Failure to properly break down tyrosine leads to abnormal accumulation of tyrosine and its metabolites in the liver, potentially resulting in severe liver disease.
Tyrosine may also accumulate in the kidneys and central nervous system.
Gaucher’s Disease: Characterized by the accumulation of a fatty substance called glucocerebroside in various organs, particularly the spleen, liver, and bone marrow. This accumulation occurs due to a deficiency of an enzyme called.
This causes these organs to enlarge and can affect their function. The fatty substances also can build up in bone tissue, weakening the bone and increasing the risk of fractures.
Wilson’s Disease: Also known as hepatolenticular degeneration, is a rare genetic disorder characterized by the accumulation of copper in various organs of the body, particularly the liver, brain, and cornea.
Dravet-Lennox Gastaut Syndrome: These are two distinct types of epileptic syndromes.
Dravet syndrome, also known as severe myoclonic epilepsy of infancy (SMEI), is a rare and severe form of epilepsy that typically begins in the first year of life.
Lennox-Gastaut syndrome is a severe form of childhood-onset epilepsy characterized by multiple types of seizures and cognitive impairment.
Rare diseases in India
As per National Consortium for Research and Development on Therapeutic for Rare Diseases, approximately 450 rare diseases have been identified and reported in India however, 80% of all rare disease patients are affected by approximately 350 rare diseases.
With an estimated burden of about 80 to 96 million cases reported annually in India.
Moreover, 70-80% of rare diseases are of genetic nature, and thus are asymptomatic, but will appear in the person’s lifetime.
In India, there are between 7000 - 8000 rare diseases, but less than 5% have therapies available to treat them.
Government Interventions
National Policy for Rare Diseases, 2021 aims at lowering the incidence and prevalence of rare diseases based on an integrated and comprehensive preventive strategy encompassing awareness generation, premarital, post-marital, pre-conception and post-conception screening and counselling programs.
Production Linked Incentive Scheme 2.0 for Pharmaceuticals, with an outlay of INR 15000 Crore providing financial stimulus to orphan drugs development under Category 1 of pharmaceutical goods in the Production Linked Incentive (PLI) Scheme.
The Central Drugs Standard Control Organisation(CDSCO) has made provisions for fast-track processing of applications for rare diseases drugs for drug trials and experimental therapies and have exempted the application fee of potential drug candidates.
Genomics for Understanding Rare Diseases: India Alliance Network (GUaRDIAN), a non-profit clinical genomics research network, has established a network of clinicians and scientists for largest clinical genomics research networks in India.
Council of Scientific & Industrial Research (CSIR), established an Indian Genetic Disease Database (IGDD) for keeps track of mutations in the causal genes for genetic diseases common in India and provides valuable insights to physicians and researchers.
Context: CCRAS under Ministry of Ayush has launched AGNI Initiative to promote innovations by Ayurveda Practitioners.
About AGNI Initiative
AGNI stands for Ayurveda Gyan Naipunya Initiative (AGNI).
It has been launched by Central Council for Research in Ayurveda Sciences (CCRAS) under Ministry of Ayush.
This initiative aims to promote research for mainstreaming the pragmatic Ayurveda practices through scientific validation and evidence based appraisal.
Under the initiative, CCRAS will document and publish the reported medical practices and therapeutic regimens for education and academic purposes in consultation with NCISM (National Commission for Indian System of Medicine).
Objective of AGNI Scheme:
Provide a platform for Ayurveda practitioners to report their innovative practices and experiences in various disease conditions along with promoting the culture of evidence based practice among Ayurveda Practitioners.
Promote culture of reporting evidence based practice among Ayurveda Practitioners.
Undertake research for mainstreaming pragmatic through scientific validation and evidence based appraisal.
Research studies may be taken up by CCRAS on the reported medical practices for mainstreaming and scientific validation by developing research proposals in collaboration with Ayurveda Practitioners and other relevant institutes/organisations.
About CCRAS
Central Council for Research in Ayurveda Sciences (CCRAS) is an apex research organisation body committed to undertaking, coordinating, formulating, development and promotion of research on scientific lines in Ayurveda.
It is under the Ministry of Ayush.
To boost scientific research through Ayurveda colleges and hospitals, CCRAS has initiated:
SPARK Program: Studentship Program for Ayurveda Research Ken (SPARK) for undergraduate scholars
PG-STAR Program: Scheme for Training in Ayurveda Research for PG Scholars
SMART Program: Scope for Mainstreaming Ayurveda in Training Professionals (SMART) Program for teachers.
Context: According to the National Organ and Tissue Transplant Organization (NOTTO), four out of five organ recipients in India between 1995 and 2021 were men.
About NOTTO
It is a National level organisation set up under Directorate General of Health Services, Ministry of Health and Family Welfare.
It functions as an apex organisation for activities related to procurement, allotment and distribution of organs in the country.
It has two divisions: (a) National Human Organ and Tissue Removal and Storage Network; (b) National Biomaterial Centre.
National Human Organ and Tissue Removal and Storage Network
It functions as apex centre for all India activities of coordination and networking for procurement and distribution of organs and Tissues and registry of organs and tissues donation and transplantation in the country.
This has been mandated as per the Transplantation of Human Organs (Amendment) Act 2011.
National Biomaterial Centre/ National Tissue Bank
The main thrust & objective of establishing the centre is to fill up the gap between ‘Demand’ and ‘Supply’ as well as ‘Quality Assurance’ in the availability of various tissues.
The Transplantation of Human Organs (Amendment) Act 2011 has included the component of tissue donation and registration of tissue Banks.
Context: Tuberculosis (TB) remains the world’s second leading cause of death from a single infectious agent, and global TB targets have either been missed or remain. The net reduction from 2015 to 2022 was 8.7%, far from the WHO End TB Strategy milestone of a 50% reduction by 2025 according to WHO’sGlobal TB Report 2023.
Key findings of the report
In 2022, the global number of new TB diagnoses reached 7.5 million, marking the highest figure since the World Health Organization (WHO) initiated its global TB monitoring efforts in 1995. This exceeded the pre-COVID baseline and the previous historical peak of 7.1 million cases in 2019, showing a significant increase from the 5.8 million cases reported in 2020 and 6.4 million in 2021.
India, Indonesia and the Philippines, which collectively accounted for nearly 60% of the reduction in the number of people newly diagnosed with TB in 2020 and 2021, recovered to above 2019 levels in 2022.
TB caused an estimated 1.30 million deaths in 2022, again almost back to the level of 2019. COVID-related disruptions are estimated to have resulted in almost half a million excess deaths from TB in the three years 2020–2022.
Treatment success rates have improved to 88% for people treated for drug-susceptible TB and 63% for people with Multidrug- and rifampicin-resistant tuberculosis (MDR/RR-TB).
The net reduction in the global number of deaths caused by TB from 2015 to 2022 was 19%, far from the WHO.
Thirty high TB burden countries accounted for 87% of the world’s TB cases in 2022 and two-thirds of the global total was in eight countries: India (27%), Indonesia (10%), China (7.1%), the Philippines (7.0%), Pakistan (5.7%), Nigeria (4.5%), Bangladesh (3.6%) and the Democratic Republic of the Congo (3.0%).
In 2022, 55% of people who developed TB were men, 33% were women and 12% were children (aged 0–14 years).
About global tuberculosis (TB) report
WHO has published a global tuberculosis (TB) report every year since 1997.
The report provides a comprehensive and up-to-date assessment of the TB epidemic, and of progress in prevention, diagnosis and treatment of the disease at global, regional and country levels.
About Tuberculosis
It is an airborne communicable disease caused by the bacteria Mycobacterium tuberculosis. Typically the bacteria grow in the body where oxygen and blood are in high amounts. As a result, 80% of TB cases are pulmonary which infect the lungs and 20% of cases are extra-pulmonary which infect the brain, uterus, stomach, mouth, kidneys and bones.
Mode of transmission: Airborne- through coughing, sneezing or spitting.
High-risk groups: People weak immunity like those infected with HIV, Under-nutrition, Diabetes, Smoking and Alcohol consumption.
Context: This editorial emphasize on ‘Ayushman Bharat Scheme’. The launch of this flagship health program i.e. Ayushman Bharat, in 2018, the Indian government has consistently emphasized the importance of enhancing medical accessibility, particularly in rural areas. This initiative aims to transform 150,000 public health centers (PHCs) into health and wellness centers (HWCs) to "bring healthcare closer to people's homes." It was evident from the beginning that achieving this goal would necessitate addressing the chronic shortages of doctors, frontline medical professionals, and healthcare infrastructure.
Given that healthcare falls under the purview of individual states in India, the central government's commitment to this endeavour necessitates a corresponding commitment from state governments. Unfortunately, most states that have traditionally lagged behind on welfare indicators have not adequately risen to this challenge.
The latest edition of the Centre’s Rural Health Statistics shows that the medical system outside urban areas continues to be plagued by a shortfall of doctors and infrastructure. Barely 45 per cent PHCs adhere to their mandate of functioning 24×7.A study published in The Lancet in February placed UP among the five states where district hospitals offer only 1 per cent of the basic services.
About Primary Health Centre (PHC)
PHCs are the cornerstone of rural health services- a first port of call to a qualified doctor of the public sector in rural areas for the sick and those who directly report or are referred from Sub-Centres for curative, preventive and promotive health care
The concept of Primary Health Centre (PHC) is not new to India. The Bhore Committee in 1946 gave the concept of PHC as a basic health unit to provide as close to the people as possible, an integrated curative and preventive health care to the rural population with emphasis on preventive and promotive aspects of health care.
The Government of India's initiative to create and expand the presences of Primary Health Centres throughout the country is consistent with the eight elements of primary health care outlined in the Alma-Ata declaration.
Examples of primary health care services include routine check-ups, immunizations, screening tests, chronic disease management, and referrals to specialists when needed. Primary health care providers can include general practitioners, nurse practitioners, midwives, and community health workers.
Why primary health care is so important
Promotes preventative care: Primary health care helps prevent illness and disease by promoting healthy living, encouraging vaccinations, and providing regular check-ups and screenings.
Increases accessibility: Primary health care is often the most accessible form of healthcare, as it is typically delivered in local clinics or health centers that are close to where people live and work.
The share of primary healthcare in Current Government Health Expenditure (CGHE) has increased from 51.3% in 2014-15 to 55.9% in 2019-20. The increased focus on primary healthcare reinforces the government’s decisions to prioritize primary healthcare in the country.
Figure: Share of Primary Health Care in Current Government Health Expenditure (%)
Reduces healthcare costs: Early detection and management of illnesses through primary health care can reduce the need for more expensive and specialized care, ultimately saving individuals and healthcare systems money.( It reduces the need for expensive secondary and tertiary healthcare.)
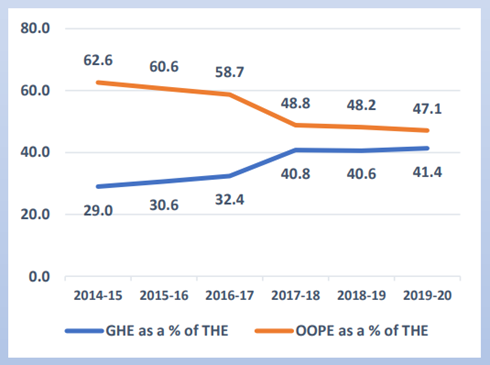
Acc to National Health Accounts Estimates for India (2019-20)- Strengthening the PHC and focusing on preventive care will reduce the Out-of-Pocket Expenditure. The share of Out-of-Pocket Expenditure (OOPE) in total Health Expenditure (THE) declined from 62.6% to 47.1%. The continuous decline in the OOPE in the overall health spending show progress towards ensuring financial protection and Universal Health Coverage for citizens.
Figure 2: Government Health Expenditure and Out-of-pocket expenditure as % of Total Health Expenditure (%)
Improves overall health outcomes: By providing comprehensive and continuous care, primary health care can help manage chronic conditions and improve overall health outcomes, including reducing mortality rates.
Addresses health inequalities: Primary health care can help address health inequalities by providing equitable access to healthcare services regardless of income, race, gender, or location.
Primary health related to Climate Change: Primary health care has an important role in responding to the climate change related threats to human health like injuries related to extreme weather events like storms, fires and floods; infectious disease outbreaks due to changing patterns of vector borne diseases; poor nutrition from reduced food availability because of drought; the psychological impact due to displacement of communities.
Primary healthcare in developed nations:The majority of developed countries' federal healthcare budgets go towards primary care, including the UK, Australia, Canada, the Netherlands, and Sweden.
Problems of PHC in India
Limited in scope- The existing primary healthcare model in the country covers only 15% of the health issues people seek care for, primarily related to pregnancy, limited childcare, and national health programs. Expanding its scope is essential for comprehensive healthcare coverage.
Funding: The funding for general healthcare is quite low, leaving insufficient funds for primary healthcare.
The central and state governments’ budgeted expenditure on healthcare touched 2.1 % of GDP in FY23 which was substantially lower that other BRICS countries (Brazil: 3.8%, China: 3.1%, Russia: 3.7%, South Africa: 4.2%)
Inadequate Infrastructure: According to the National Health Profile 2019 report, 22% of primary health centers do not have a separate room for immunization and family planning services.
In Rajasthan, the population is often so dispersed (especially in hilly areas in the south and in the desert in the west) that a family may need to travel 10-20 km to reach the nearest PHC according to an analysis by the Centre for Economic and International.
Shortage of Healthcare Professionals: The delivery of quality health services is hampered by supply shortages, inadequate management, and the absence of proper training and supervision for healthcare workers. These issues can lead to interruptions in care, inefficiency, and outdated practices, all of which impact patient well-being.
The rural healthcare infrastructure is three-tiered and includes a sub-center, primary health center (PHC) and CHC. Indian PHCs are short of more than 3,000 doctors, with the shortage up by 200% over the last 10 years to 27,421, as IndiaSpend reported in 2016.
Lack of Access to Medicines:
The high cost of medicines is a significant barrier to healthcare access in India, with many people unable to afford even basic medications.
The government's free medicines program, which provides essential medicines to patients for free, has been plagued by shortages and supply chain issues.
The lack of access to medicines has led to many patients turning to unlicensed and unregulated pharmacies, which may sell substandard or counterfeit drugs.
Poor Quality of Care:
A study published in the Lancet found that around 50% of patients in India do not receive the appropriate care for their health conditions.
The lack of quality healthcare services is due to a range of factors, including a shortage of qualified healthcare professionals, inadequate infrastructure, and poor regulation of healthcare providers.
In addition, many patients in India lack awareness about their health conditions and may not seek timely medical treatment, leading to complications and poor health outcomes.
An analysis by the Centre for Economic and International - India has a large network of primary health centres (PHCs), each supposed to serve a population of 25,000. In many poor states, such as Madhya Pradesh, Bihar and Jharkhand, however, a PHC covers as many as 45,000, 49,000 and 76,000 people.
Under-investment in primary healthcare : also means that PHCs continue to remain under-equipped and lacking supplies and drugs to provide comprehensive primary care.
For example, of the 709 PHCs surveyed in 2009 by the International Institute for Population Sciences, Mumbai, about 24% did not have an electricity connection and 63% did not have piped water supply.
At the same time, PHCs are expected to deliver centrally designed, targeted vertical programs, alienating them further from communities. As a result, even those families that can access PHCs continue to look elsewhere for their critical healthcare needs.
Urban Neglect in Indian Healthcare System: The primary healthcare system in India has historically overlooked the growing urban population, as its focus has mainly been on rural areas. This neglect stems from historical policies and infrastructure designed for rural regions, despite the increasing urban population.
Way Forward
Srinath Reddy committee recommendation: The High-Level Expert Group (HLEG) on Universal Health Coverage (UHC) headed by K. Srinath Reddy recommended that expenditures on primary health care, including general health information and promotion, curative services at the primary level, screening for risk factors at the population level, and cost-effective treatment, targeted toward specific risk factors, should account for at least 70% of all health care expenditures.
Ayushman Bharat scheme seeks to upgrade more than 1.5 lakh health facilities like Sub Centres and Primary Health Centres to health and wellness Centres (HWC). These centres would deliver Comprehensive Primary Health Care (CPHC) bringing healthcare closer to the homes of people. This has to be implemented properly.
Telemedicine: Telemedicine provides patients remote access to medical consultations and treatments via telecommunications technology. In turn, this contributes to closing the gaps in healthcare access, particularly in rural and remote areas. Telemedicine has proven to be a boon for Indians during the uncertain times of lockdowns, and it has the potential to make remote, optimized healthcare accessible to every corner of India in the future.
Health Information Exchange (HIE): HIE systems enable the seamless sharing of patient health information between various healthcare providers, enhancing care coordination and substantially reducing medical errors.
Mobile Health (mHealth): mHealth is an emerging concept involving the utilization of mobile devices and technology for health services, such as appointment scheduling, remote monitoring, and medication reminders. It can significantly improve patient access to care and treatment plan adherence.
Government must increase budgetary allocations to healthcare to at least 3-4% of GDP so that public expenditure on healthcare is at least 70% of total health expenditure.
Context: The Food Safety and Standards Authority of India (FSSAI) has recommended the inclusion of QR code on food products for accessibility by visually impaired individuals under its Food Safety and Standards (Labelling and Display) Regulations 2020.
About QR Code on Food Labels to help visually disabled
The information on food labels includes product name, shelf life, nutrition facts, vegetarian/non-vegetarian logos, ingredient lists, allergen warnings, and other product specific labelling requirements.
This information aims to help consumers make informed food choices and ensure safe food access for all, including individuals with special needs like the visually impaired.
It will also provide inclusive access to information, guaranteed by Article 19 as a fundamental right of citizens.
Furthermore, this will complement The Rights of Persons with Disabilities Act 2016, which acknowledges the needs and rights of people with disabilities and places a strong emphasis on accessibility and the promotion of their health.
About Food Safety and Standards (Labelling and Display) Regulations 2020
The regulations prescribe the labelling requirements of pre-packed foods and display essential information about premises where food is manufactured, processed, served, and stored.
The non-veg symbol shall consist of a brown colour-filled triangle inside a square with a brown outline having sides not less than the minimum size specified in the regulation.
Recommended Dietary Allowance (RDA) is mandatory to be displayed on the label.
Mandatory declaration of allergen information.
Some new logos were established to identify foods with different categories, such as for Fortified Foods, organic foods.
E-commerce platforms are required to provide for mandatory labelling of food products offered for sale through their platform with certain exceptions.
Also included restaurant operators with large networks of chains within its scope.
About FSSAI
Body: Statutory body under the Food Safety and Standards Act 2006.
Nodal Ministry: Ministry of Health & Family Welfare.
Headquarters: Delhi
Replaced various acts: Prevention of Food Adulteration Act, 1954, Fruit Products Order, 1955, Meat Food Products Order, 1973, Vegetable Oil Products (Control) Order, 1947, Edible Oils Packaging (Regulation)Order 1988, Solvent Extracted Oil, De- Oiled Meal and Edible Flour (Control) Order, 1967, Milk and Milk Products Order, 1992 etc. were repealed after commencement of FSS Act, 2006.
Appointment of chairperson and CEO: By Government of India.
Objective: Responsible for protecting and promoting public health through the regulation and supervision of food safety.
Context: A draft menstrual hygiene policy is out by Ministry of Health and Family Welfare.
Need for Menstrual Hygiene Policy policy
Health and Hygiene: Poor menstrual hygiene can lead to various health issues, including infections and discomfort. According to 5th NHFS (2019-2021):
Women aged 15-24 years who use a hygienic method of protection during their menstrual cycle is 78%. Among these women, 64% use sanitary napkins, 50% use cloth, and 15% use locally prepared napkins.
Only 73% of rural women while 90% of urban women use a hygienic method of menstrual protection respectively.
However, a few States continue to have lower than average access to use of a hygienic method of menstrual protection by women and girls.
Dignity and empowerment: Access to proper menstrual hygiene products and facilities is a matter of dignity and basic human rights. It is essential to ensure that individuals can manage their menstruation with dignity, without feeling ashamed.
Gender equality: Menstruation is associated with stigma and discrimination, leading to gender inequality. A menstrual hygiene policy can help challenge these social norms and promote gender equality by addressing issues related to menstruation.
Accessibility and affordability: A policy can promote the availability and affordability of menstrual hygiene products.
Promote work participation: By creating a more inclusive and supportive environment like, may include flexible working hours, access to sanitary products, and menstrual leave. It will reduce absenteeism and increase productivity and higher work participation rates.
Access to education: By providing essential menstrual hygiene products and support, schools and institutions can help remove barriers that might otherwise prevent girls from attending classes.
About draft Menstrual Hygiene Policy
Menstrual hygiene is the practice of maintaining cleanliness and managing menstruation in a safe and healthy way. It is important for the well-being and dignity of individuals who menstruate. Proper menstrual hygiene management helps prevent infections, discomfort, and allows individuals to continue their daily activities without disruption.
Ministry of Health and Family Welfare(MoHFW) is the Nodal Ministry for the Menstrual hygiene policy.
The policy recognizes menstruation as a natural bodily process for all who menstruate including girls and women of reproductive age and addresses the long-standing challenges associated with menstruation in our country.
By adopting a life cycle approach, the policy ensures comprehensive support through the entire menstrual journey, recognizing the unique needs of individuals from menarche to menopause.
Specific focus on prioritising underserved and vulnerable populations, ensuring equitable access to menstrual hygiene resources and addressing their specific needs.
This policy aligns with India’s commitment to achieving the Sustainable Development Goals (SDGs), particularly in relation to Goal 3 on good health and well-being, Goal 4 on quality education, Goal 5 on gender equality, and Goal 6 on clean water and sanitation.
The policy will serve as a catalyst to raise awareness, challenge societal norms and foster a society that embraces menstrual hygiene as a natural and normal part of life.
Vision
All women, girls and persons who menstruate are able to experience menstruation in a manner that is safe, healthy and free from stigma.
Goal
Each girl, woman and person who menstruates across India can access safe and dignified menstrual hygiene resources in order to improve their quality of life and thereby realize their full potential in health and wellbeing, education, economic and other aspects of life.
Target
The policy caters to the needs of and covers all who menstruate in rural, urban and tribal areas, as well as in educational institutions, workplaces, healthcare settings and other public places.
Objectives
To ensure that women, girls and persons who menstruate have access to safe, hygienic and quality menstrual products and sanitation facilities.
To create an enabling environment for people including women, girls, men and boys so that they have access to correct information on menstruation, and to address myths, stigma and gender issues around menstruation.
To provide a coordination mechanism among different Central Government Ministries, States/ UTs and relevant stakeholders and sectors.
To create a ‘menstrual friendly environment’ in all settings including homes, schools/ educational institutions, workplaces and public spaces.
To foster innovative practices with social entrepreneurs and the private sector.
To strengthen environmentally sustainable menstrual waste disposal.
Policy strategy
Ensure access to affordable and safe menstrual hygiene products: To ensure affordable and accessible menstrual products such as disposable or reusable sanitary pads, menstrual cups, tampons or reusable cloth pads, etc are available to all who menstruate, especially those in low-income communities and marginalized groups.
Promote quality standards and regulatory framework: Develop and implement comprehensive quality standards for different types of menstrual hygiene products available in the market to ensure their safety, efficacy and reliability.
Availability of clean and dignified menstrual hygiene facilities: Promote the development and improvement of menstrual-friendly infrastructure in homes, educational institutions, workplaces and public spaces to include safe, clean and private toilets, proper waste disposal systems and handwashing facilities with soap and clean water.
Promotion of education and awareness on menstrual hygiene: Awareness campaigns targeting menstruators to provide accurate information including options of products available, debunk myths and misconceptions and address social and gender-related challenges associated with menstruation.
Collaboration with Non-government sector/engagement with private sector: Support research and development initiatives that explore new technologies, materials and product designs which improve menstrual hygiene management, while considering accessibility, ease of use, affordability and environmental sustainability.
Foster research and innovation in menstrual hygiene management: Encourage research institutes and academia to contribute to evidence-based policymaking, promote innovation and improve the overall understanding and implementation of menstrual hygiene practices.
Context: The use of quality generic medicines holds plenty of promise to reduce the burden on the common man. However, India needs to ensure people have access to quality generic drugs.
About Generic Drugs
Generic Drugs refer to a medication that is equivalent to a brand-name product in terms of its active ingredient, strength, dosage form, and intended use.
It is marketed either by a salt or brand name. They have the same potency, quality, and implications and work in an identical manner as the branded medicine.
India is the largest producer of generic drugs globally.
Need for generic drugs
Reduce Out-of-Pocket Expenditure: In India,around 94 million people are pushed into poverty due to expenditure on healthcare. About two-thirds of the expenditure is incurred on medicines.
Accessibility, availability and affordability: It may become available once the patent on the brand-name drug expires. This allows for competition in the pharmaceutical market, which often results in lower prices for consumers. This makes generic medicines price 30% to 70% less than branded medicines.
Effectiveness: It works in the same way as their brand-name counterparts. They have the same intended use and are equally effective.
Rise in the number of fatal diseases: It has increased over the years and the cost of medicines for such diseases is very high.
Challenges to generic drugs
Falsified and counterfeit drugs: Due to lack of transparency in the licensing procedures of Drugs, and lack of quality facility, it has resulted in the increased supply of low-quality, spurious and substandard drugs.
In 2018, the Central Drug Standard Control Organization (CDSCO) identified nearly 4.5 per cent of all generic medicines in the domestic market to be substandard due to lack of testing facilities.
Counterfeit products have entered the supply chain with severe consequences, as seen in Gambia and Uzbekistan.
Absence of appropriate scientific standards: Doctors do not prescribe a generic drug due to their lack of trust in the quality available in the Indian market, which lacks scientific standards in India.
Lack of resources and manpower:Drug control procedures in India suffer from a lack of resources and manpower. Widespread corruption within the system makes matters worse.
Problem of naming a fixed-dose combination (FDC): Many fixed-dose combinations (FDCs) drugs contain even 8 or 9 Active Pharmaceutical Ingredients. To prescribe a generic name for each of the eight or nine ingredients is a very tedious and impractical task.
Government Initiatives
Guidelines by the National Medical Commission (NMC) make it mandatory for doctors to write generic drug names legibly and preferably in capital letters.
Pradhan Mantri Bhartiya Janaushadhi Pariyojana (PMBJP): To provide quality generic medicines at affordable prices. Prices of medicines sold through these outlets are 50-90% less than that of branded medicine prices in the open market.
Free Drugs Service Initiative (FDSI) 2015: It was launched under the National Health Mission (NHM) on procurement of generic essential medicines at low prices, eliminating irrational medicines and unscientific fixed-dose combinations.
Drugs Technical Advisory Board (DTAB) has recommended that retailers should maintain a separate rack/shelf solely for the storage of generic medicines sold in the proper name.
Way Forward
Utilising anti-counterfeiting technologies for counterfeit drugs: Through imaging technologies, variable data printing of unique numbers or barcodes with speciality inks, including invisible inks, and with RFID.
Strong regulatory framework: Strengthen and enforce regulations that ensure the safety, quality, and efficacy of generic medicines. Create a clear approval process for generic drugs to enter the market.
Drugs Controller General of India need to work in close association with the pharmaceutical companies and local drug control authorities to combat the menace of counterfeit drugs.
Research and Development Support: Provide grants or incentives to pharmaceutical companies to invest in research and development of generic versions of essential medicines.
Pharmacy Incentives: Reward pharmacies for promoting and dispensing generic medications.
API Sourcing: Ensure the sourcing of APIs from reputable and approved manufacturers, preferably those that adhere to Good Manufacturing Practices (GMP) to ensure the quality of drugs.
Context: Outrightly denying traditional medical systems would be a hasty dismissal of valuable medical experience and a disservice to the scientific attitude. India needs to work on evidence-based traditional medicine. The acceptability of traditional medicines in the scientific community would increase if evaluated by the methods of modern science in a way that does not compromise with the wholeness of Ayurvedic formulations.
Evidence-based medicine vs traditional medicine
Evidence-Based Medicine (EBM): EBM is based on the integration of the best available scientific evidence, clinical expertise, and patient preferences and values. It is based on empirical data rather than anecdotal evidence.
Traditional Medicine: Rooted in tradition and experience, traditional medicine is based on long-standing practices passed down through generations. It may include herbal remedies, cultural rituals, and practices.
Reasons for non-development of alternate medicine in India
Lack of scientific validation: Alternative medicine is often not based on scientific evidence or rigorous testing. Without proper scientific validation, it can be difficult for alternative medicine to gain acceptance in the medical community and among the general public.
Limited government support: While India has a rich tradition of alternative medicine, government support for research and development in this field, in the past has been limited, which has hindered the growth of alternative medicine. E.g., Lack of dedicated funding mechanisms for research and development of alternative medicine.
Competition from conventional medicine: Conventional medicine, including modern pharmaceuticals, is highly developed and widely accepted in India. This has made it difficult for alternative medicine to gain a foothold and compete in the marketplace.
Lack of standardisation: Unlike conventional medicine, which is highly standardised and regulated, alternative medicine often lacks standardisation. This can lead to inconsistencies in the quality and efficacy of alternative treatments, which can undermine public confidence in these therapies.
Scepticism among medical professionals: Some medical professionals remain sceptical about the efficacy of alternative medicine, particularly when it comes to treating serious or life-threatening conditions.
Recent developments
The government has established the Department of Ayurveda, Yoga and Naturopathy, Unani, Siddha, and Homoeopathy (AYUSH) to promote the integration of traditional Indian medicine with modern medicine.
In May 2023, a Memorandum of Agreement was signed between the Indian Council of Medical Research (ICMR) and the Ministry of AYUSH for collaboration and cooperation in health research in the field of Integrated Medicine.
Integrated medicine in India refers to the practice of combining traditional Indian medicine systems, such as Ayurveda, Yoga, Unani, Siddha, and Homeopathy (AYUSH), with modern medicine.
Aim: To provide patients with a holistic approach to healthcare that takes into account physical, mental, emotional, and spiritual aspects of health. By combining different therapies, healthcare providers can tailor treatment plans to individual patients.
The Ministry of AYUSH and ICMR have joined hands to undertake quality human clinical trials to generate evidence on the benefits of using Ayurveda along with modern medicine (evidence-based medicine) in treating certain disease conditions of national importance.
ICMR will design and conduct these trials as it holds decades of experience in conducting human clinical trials. In the initial phase, the collaboration will be restricted to Ayurveda.
Yoga, Unani, Siddha and Homoeopathy may be included in future and each system will be tested together with modern medicine.
Significance of the fusion of the traditional Indian medicine system with modern medicine:
The recent COVID-19 Pandemic has underscored the importance of AYUSH thus calling for its revival and fusion with modern medicine to build a holistic health system, which provides:
Comprehensive care: Traditional Indian medicine, such as Ayurveda, focuses on a holistic approach to health and wellness. This means that it considers the individual as a whole, including physical, mental, and emotional factors. By combining this approach with modern medicine, patients can receive more comprehensive and personalized care.
Accessibility: Traditional Indian medicine is often more accessible and affordable than modern medicine. By incorporating these therapies into modern healthcare systems, it reduces out-of-pocket expenditure.
Innovation: By combining traditional Indian medicine with modern medicine, new and innovative treatments can be developed, which can lead to better healthcare outcomes for patients and advances in medical research.
Overcome the challenge of doctors’ shortage: The existing doctor-patient ratio in India is 1:1700 and the ratio improves to around 1:800 (below the WHO’s mandate of 1:1000) with the integration of the AYUSH practitioners.
Help tackle multidrug-resistant diseases such as tuberculosis, lifestyle disordersand long-term diseases. It can reduce the growing burden of non-communicable diseasessuch as cardiovascular diseases- The WHO Report highlights that non-communicable diseases account for 63% of deaths in India.
Reduces the pollutionin the manufacturing and waste management of allopathic medicine.
Steps to build a holistic health system:
Invest in research and development of AYUSH for integration with modern medicine.
Update curriculum in medical courses to integrate traditional Indian medicine system with modern medicine.
Introduce bridge courses for AYUSH practitioners and health professionals for interdisciplinary learning.
Co-locate AYUSH facilities in hospitals and primary health centres.
Build awareness in the Public about the benefits and limitations of integrated medicine through public health campaigns, community outreach programs, and partnerships with traditional healers and practitioners.